In the world of geriatrics and rehabilitation, few tools have been as transformative as the Clinical Frailty Scale (CFS). Developed by Dr. Kenneth Rockwood and his colleagues at Dalhousie University, this tool shifted the medical community’s focus from counting birthdays to assessing actual function. It provides a standardized language for something we often recognize intuitively but struggle to quantify: the state of frailty.
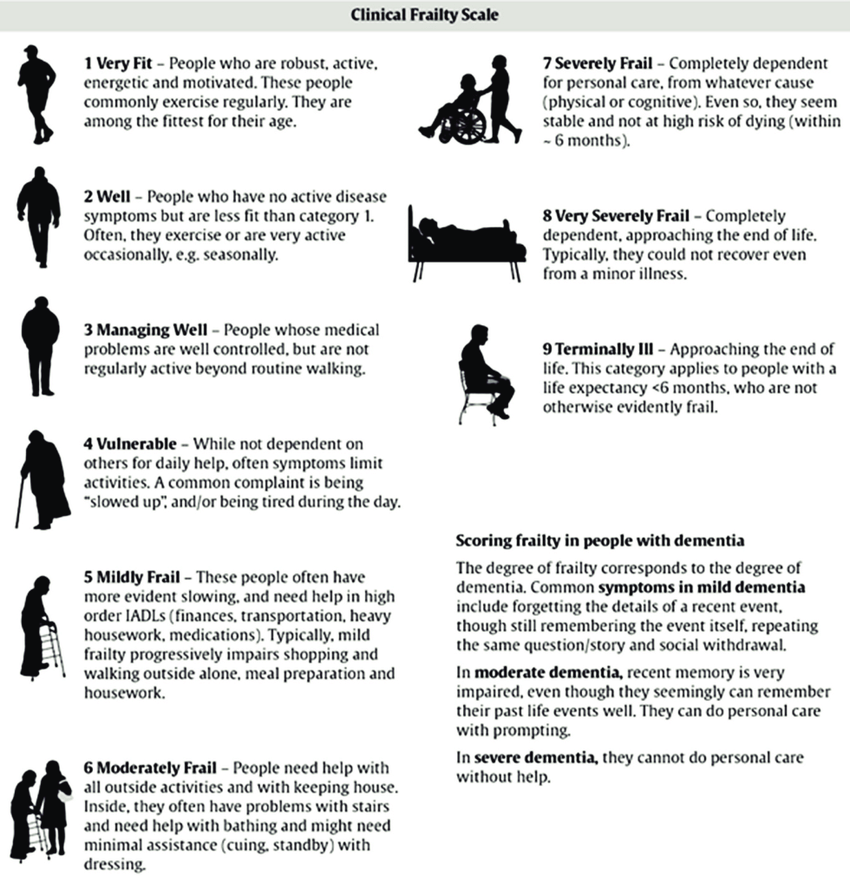
Dr. Rockwood, a geriatrician and professor, recognized that chronological age is often a poor indicator of health. Two people aged 80 can present vastly different clinical pictures. One might be hiking weekly, while the other requires assistance for basic self-care. The Clinical Frailty Scale was created to bridge this gap. It is a 9-point scale that categorizes a person’s level of fitness or frailty based on their daily activity and functional independence.
How Clinicians and Therapists Use the Scale
For medical and rehabilitation professionals, the CFS is not just a label. It is a roadmap for treatment planning. It allows multidisciplinary teams to speak a common language regarding a patient’s physiological reserve.
Doctors and Specialists Physicians use the scale to guide critical decisions. It helps them predict how a patient might tolerate a surgery or a new medication. For a patient who is “Very Fit” (Score 1), a doctor might pursue aggressive treatment options similar to those for a younger adult. Conversely, for a patient scoring higher on the scale, the focus might shift toward conservative management or prioritizing quality of life over invasive procedures.
Physiotherapists and Occupational Therapists For rehab therapists, the CFS is integral to setting realistic, person-centred goals.
- Physiotherapists use the scale to assess physical reserve. If a patient is “Mildly Frail” (Score 5), the physiotherapist knows that while mobility is limited, there is potential to regain strength and balance. They design exercise programs specifically to prevent progression to a higher frailty score.
- Occupational Therapists (OTs) look at the functional implications of the score. An OT uses the scale to evaluate Activities of Daily Living (ADLs). If a patient is “Moderately Frail” (Score 6), meaning they need help with outside activities and keeping house, the OT focuses on home modifications, energy conservation techniques, and prescribing the right assistive technology to maintain independence.
This alignment is crucial for teams like Lifeweavers, where the goal is providing an ultra holistic approach to rehab therapy. By understanding exactly where a client sits on the scale, the team can integrate their diverse expertise to create a seamless support network.
The Role of the Public: Awareness vs. Assessment
The Clinical Frailty Scale is famous for its visual simplicity. It uses pictures and short descriptions that allow laypeople to roughly estimate where a loved one might stand. This accessibility makes it an excellent tool for self-informed awareness.
Families can use the descriptions as a “check engine” light. If you notice a parent moving from “Managing Well” (Score 3) to “Vulnerable” (Score 4), it serves as an early warning system. It signals that functional decline has started and that it is time to intervene before a crisis occurs. This aligns with the philosophy that prevention is at the heart of what good rehab therapists do.
However, self-assessment has limitations. The public should view the CFS as a prompt to seek professional help rather than a tool for diagnosis. Here is why working with a registered rehab therapist is essential:
- Nuance and Accuracy: A registered therapist is trained to distinguish between temporary illness and true baseline frailty. They ensure the score accurately reflects the person’s usual state, not just a bad day.
- Hidden Factors: Clinicians dig deeper than the visual cues. They assess cognitive status, nutritional health, and muscle mass (sarcopenia) which might not be immediately visible to family members.
- Actionable Plans: Knowing the score is only the first step. A therapist knows what to do with that information. They build the bridge between “surviving” and “thriving” by designing interventions that can halt or sometimes reverse the trajectory of frailty.
Dr. Rockwood’s scale teaches us that frailty is not an inevitable consequence of ageing. It is a dynamic state. By using the CFS to identify issues early and partnering with registered therapists, families can ensure that a long life is accompanied by the ability to enjoy it.